Diagnosis
Endometriosis cannot be diagnosed by symptoms alone. Your physician may suspect endometriosis if you are having fertility problems, severe menstrual cramps, pain during intercourse, or chronic pelvic pain. It also may be suspected when there is a persistent ovarian cyst. Endometriosis is often found in close family members like a mother or sister. Remember, however, that many women with endometriosis have no symptoms at all.
Pelvic Exam

Pelvic exam
|
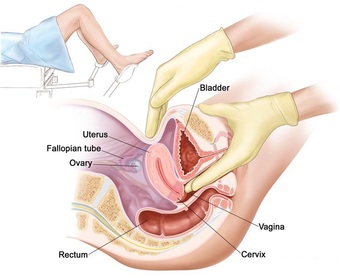
Bimannual Pelvic Exam
|
Certain findings of a pelvic examination may lead your physician to suspect endometriosis. The doctor, during bi-manual pelvic exam, may feel a tender nodule behind the cervix during a combined vaginal and rectal exam, or the uterus may be tilted back or retroverted. One or both ovaries may be enlarged or fixed in position. Occasionally, endometriosis implants may be visible in the vagina or the cervix. Although your physician may suspect endometriosis, based on your history and the results of a pelvic exam, surgery is needed to confirm endometriosis.
Laparoscopy
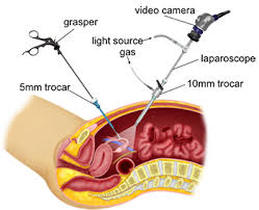
Laparoscopy is an outpatient surgical procedure that enables the physician to see the pelvic organs and look for endometriosis. During laparoscopy, a thin camera called a laparoscope is inserted into the abdomen through a small incision near the navel. The laparoscope allows the surgeon to see the surface of the uterus, fallopian tubes, ovaries, and other pelvic organs.
The extent of endometriosis is evaluated during laparoscopy. A clinical staging system is used to describe the extent of endometriosis, adhesions, and endometrioma cysts in the ovary. A score of 1-15 indicates minimal or mild endometriosis and a score of 16 or higher indicates moderate or severe disease. The staging system, however, does not correlate well with a woman’s chance of conceiving with fertility treatment or the degree of pain that she experiences.
Your physician may decide to treat your endometriosis during the laparoscopy. Additional small incisions allow your physician to insert surgical instruments. Endometriosis may be coagulated, vaporized, burned, or excised, and scar tissue or ovarian cysts may be removed. During laparoscopy, your doctor can determine if your fallopian tubes are open by injecting dye through the cervix into the uterus. If the tubes are open, the dye will flow out the ends of the fallopian tubes.
The extent of endometriosis is evaluated during laparoscopy. A clinical staging system is used to describe the extent of endometriosis, adhesions, and endometrioma cysts in the ovary. A score of 1-15 indicates minimal or mild endometriosis and a score of 16 or higher indicates moderate or severe disease. The staging system, however, does not correlate well with a woman’s chance of conceiving with fertility treatment or the degree of pain that she experiences.
Your physician may decide to treat your endometriosis during the laparoscopy. Additional small incisions allow your physician to insert surgical instruments. Endometriosis may be coagulated, vaporized, burned, or excised, and scar tissue or ovarian cysts may be removed. During laparoscopy, your doctor can determine if your fallopian tubes are open by injecting dye through the cervix into the uterus. If the tubes are open, the dye will flow out the ends of the fallopian tubes.
Other Diagnostic Procedures
In special cases, your doctor may use special imaging techniques such as ultrasound, computerized tomography (CT) scan, or magnetic resonance imaging (MRI) to gather more information about your pelvis. These procedures can identify cysts and help characterize the fluid within an ovarian cyst, although an endometriotic cyst and a normal corpus luteum cyst may have a similar appearance. These tests are useful when evaluating women experiencing infertility and/or chronic pelvic pain.
